
Biofilm and susceptibility language is most useful when it keeps the organism, model, exposure, endpoint, and author-defined term attached to the source.
This article helps researchers read octenidine biofilm, tolerance, adaptation, reduced-susceptibility, and resistance statements with enough method context to understand what the evidence actually supports.
Quick Position
Biofilm studies can support source-specific statements about tested organisms, surfaces, concentrations, exposure times, and endpoints. They do not, by themselves, support statements that an octenidine product treats biofilm infection, prevents device infection, or performs the same way in a wound, mucosal site, catheter, or clinical protocol.
Reduced susceptibility language needs the same care. A paper may measure MIC, MBC, survival after a short exposure, serial passage adaptation, gene carriage, or association with antiseptic use. Those are not interchangeable endpoints. When a source uses the word “resistance,” preserve the author’s meaning and then explain the method that supports it.
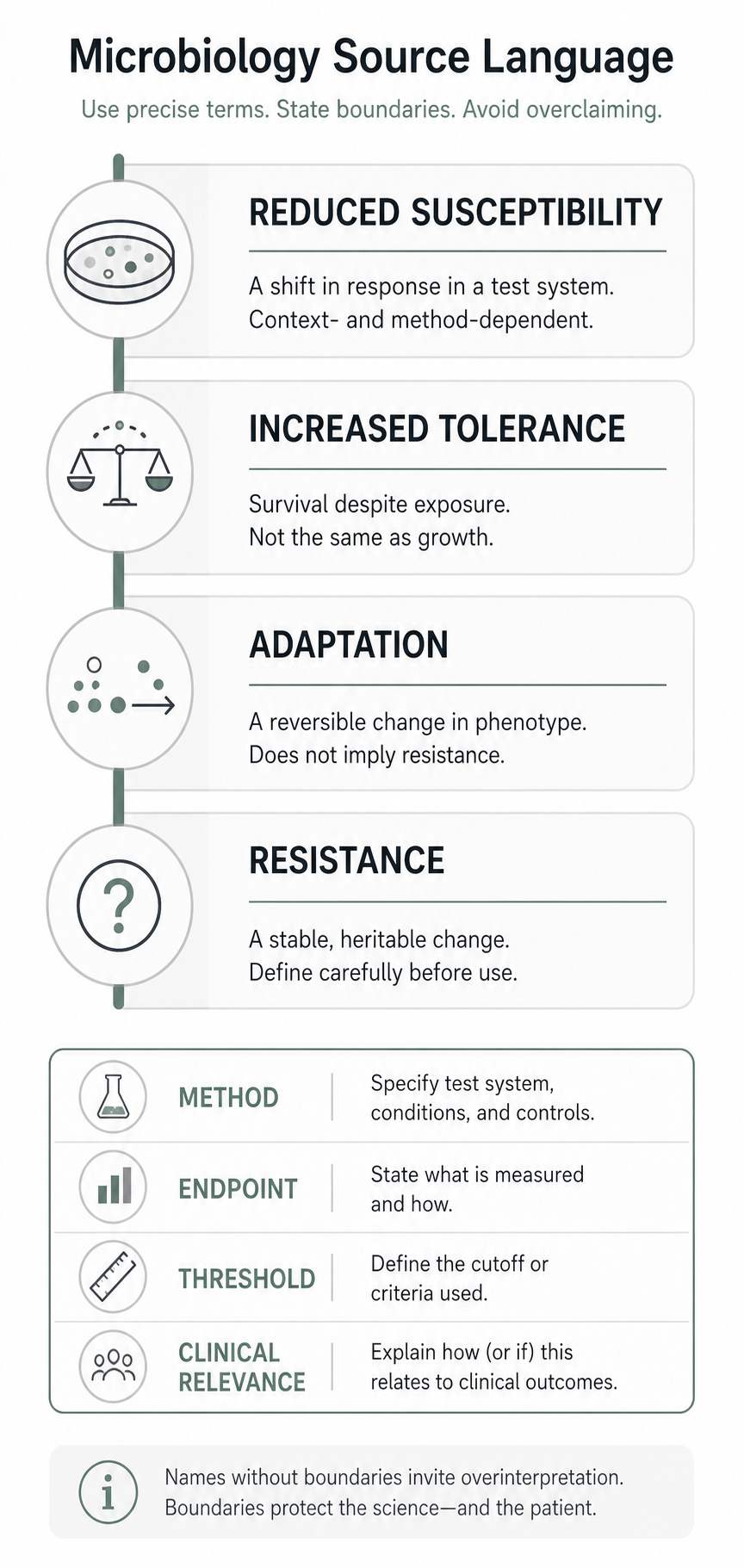
The most cautious default wording is usually “reduced susceptibility,” “increased tolerance,” or “adaptation” until the article has named the organism, method, endpoint, and threshold.
Keep The Substance Name Attached To The Source
Official identity records are the starting point for naming. PubChem lists CID 51166 as octenidine hydrochloride and maps the salt-style formula to octenidine dihydrochloride language. FDA GSRS lists UNII U84956NU4B under the preferred name “OCTENIDINE HYDROCHLORIDE” and includes “OCTENIDINE DIHYDROCHLORIDE” among its synonyms.
That identity mapping is useful, but it does not make every paper, formulation, product, concentration, or exposure design equivalent. A biofilm paper using “octenidine hydrochloride” and an adaptation paper using “octenidine” may be close enough for document matching, but each claim should keep the source’s own term visible.
Biofilm Findings Are Model Findings
Biofilms are often more difficult to interpret than planktonic-culture results because the model changes the question. A general biofilm review describes biofilm recalcitrance as involving antimicrobial tolerance, immune-response tolerance, and possible development of resistance mechanisms. That review is not octenidine-specific, but it explains why biofilm claims should name the model before making a conclusion.
The 2014 Pathogens study on octenidine hydrochloride tested Staphylococcus aureus, MRSA, and VRSA biofilms on polystyrene plates, stainless steel coupons, and urinary catheters. The study used defined millimolar octenidine hydrochloride concentrations, included presence or absence of serum protein, measured viable counts, and used confocal microscopy to assess biofilm architecture. The authors reported rapid inactivation under those in vitro conditions.
The 2016 Frontiers in Microbiology study tested octenidine dihydrochloride against Acinetobacter baumannii biofilms on polystyrene, stainless steel, and urinary catheters. The study used concentrations reported as 0.3%, 0.6%, and 0.9% with corresponding millimolar values, and it included confocal and scanning electron microscopy. Those details make the paper useful for a model-system statement, not for a patient-care conclusion.
How To Write A Biofilm Claim
For a biofilm source, the claim should include the method boundary:
- Name the organism and strain or isolate group.
- Name the biofilm model, such as polystyrene plate, stainless steel coupon, catheter segment, agar-disc system, or other surface.
- State whether the study tested biofilm prevention, treatment of established biofilm, planktonic killing, or a mixed endpoint.
- Include concentration, exposure time, temperature, medium, protein or serum condition, and formulation if the source provides them.
- Name the endpoint, such as viable count reduction, MIC, MBC, microscopy, biofilm architecture, or growth curve.
- State the limitation in the same paragraph when a reader could mistake the result for clinical effectiveness.
That structure is intentionally repetitive. Biofilm language becomes unsafe when it drops the model and keeps only the result.
Tolerance, Adaptation, And Resistance Are Not One Word
Disinfectant and antiseptic terminology is less settled than antibiotic breakpoint language. The CDC disinfection guideline explains a common distinction: reduced susceptibility or increased tolerance to disinfectants does not necessarily mean disinfectant failure, because in-use concentrations may still be above cidal levels. That source is broad disinfection guidance, not octenidine-specific, but it is a useful warning against importing antibiotic-resistance language too quickly.
The Nature Reviews Microbiology review on disinfectants and antiseptics describes biocide action and resistance as shaped by intrinsic mechanisms, acquired mechanisms, inappropriate or low-concentration exposure, and biofilm context. For octenidine writing, the practical step is to identify which susceptibility method the source used. Framing resistance as either fully present or impossible misses the question the source actually answered.
Use “adaptation” when a study repeatedly exposes organisms and then measures changed susceptibility or survival. Choose “reduced susceptibility” when a study reports higher MIC, MBC, or related values compared with a reference or earlier population. “Increased tolerance” fits when the source frames the result as survival at a higher exposure or concentration. Reserve “resistance” for cases where the source’s definition, method, and threshold are attached.
Antiseptic Adaptation Is Not Antibiotic Resistance
“Antimicrobial resistance” is a broad phrase. In octenidine writing, it should not be used as a shortcut for antibiotic resistance unless the source actually tests antibiotic susceptibility, clinical breakpoints, or antibiotic-treatment outcomes.
Most octenidine adaptation sources ask a narrower antiseptic question: after a defined exposure history, does an organism show a higher MIC, higher MBC, greater survival after contact, changed membrane behavior, changed efflux expression, or a different response to another biocide? Those findings can matter for infection-control research and antiseptic stewardship, but they are not the same evidence as antibiotic resistance in a clinical isolate under antibiotic breakpoint rules.
The clean sentence keeps the evidence lane visible. “Repeated octenidine exposure selected for increased octenidine tolerance in this Pseudomonas aeruginosa model” is stronger than “octenidine caused antimicrobial resistance.” “This MRSA isolate set showed reduced chlorhexidine susceptibility associated with qac carriage, but did not show the same direct octenidine association” is stronger than “qac genes prove antiseptic resistance.” The first wording lets the source speak. The second imports a conclusion the source may not support.
When a source uses broad antimicrobial-resistance language, the octenidine contribution should usually be framed as antiseptic susceptibility, antiseptic tolerance, biocide adaptation, or biofilm-mediated recalcitrance. Antibiotic cross-resistance should be stated only when the source measured it and the article names the antibiotic endpoint separately from the antiseptic endpoint.
What The Pseudomonas Adaptation Papers Support
The 2018 Journal of Hospital Infection study exposed seven clinical Pseudomonas aeruginosa isolates to increasing octenidine concentrations over several days and measured fitness, MBC at different exposure times, MICs, and antimicrobial susceptibility. The same paper also tested a drain-trap population in a simulated clinical setting exposed to a diluted octenidine formulation over three months. The authors reported increased tolerance to octenidine formulations and chlorhexidine in the laboratory system and increased tolerance in the simulated setting that was lost after removing octenidine exposure.
The 2021 Communications Biology paper followed that question mechanistically. It studied octenidine-adapted P. aeruginosa and reported mutations associated with increased tolerance, including a small deletion in smvR linked to increased expression of the MFS efflux pump SmvA, and additional lipid-synthesis gene changes under higher-level adaptation. The authors also described membrane-remodelling and metabolic changes.
Those papers support language about P. aeruginosa adaptation under repeated-exposure and simulated-setting conditions. They should not be rewritten as proof that all organisms will adapt, that all octenidine products fail, or that patient outcomes are known from the model.
What The Staphylococcus Studies Add
The 2018 mBio study assembled Staphylococcus aureus isolates from before widespread chlorhexidine and octenidine use and from a UK hospital trust during changes in decolonization regimens. It reported increased MIC and MBC values for chlorhexidine during high chlorhexidine use and increased MICs and MBCs for octenidine after octenidine was introduced. The authors did not report apparent cross-resistance between the two agents, and susceptibility did not correlate simply with qac efflux-pump gene carriage.
The 2019 Clinical Microbiology and Infection study gives a different kind of evidence. It was a serial cross-sectional study of 878 MRSA isolates from a healthcare network. The authors reported associations between antiseptic exposure and qacA/B carriage, and between chlorhexidine exposure, qac genes, and reduced chlorhexidine susceptibility. They did not find a direct association between octenidine exposure and reduced octenidine susceptibility, or between reduced octenidine susceptibility and qacA/B or qacC carriage.
Together, those studies make the article’s wording more cautious. qac gene carriage should not be treated as automatic octenidine resistance. A change in MIC or MBC should not be treated as clinical failure. A negative association in one surveillance study should not be treated as proof that reduced octenidine susceptibility cannot emerge.
Experimental Setup Can Change The Result
The 2022 Antibiotics paper on octenidine efficacy is useful because it shows how laboratory setup can affect interpretation. In Escherichia coli experiments, the authors reported that octenidine activity depended on experimental conditions such as solvent and bacterial concentration. That kind of finding is not a biofilm or surveillance result, but it reinforces the same editorial rule: do not separate a susceptibility number from the experimental setup that produced it.
A source-specific susceptibility statement should normally carry at least four pieces of context: active term, organism, method, and endpoint. If the statement compares two sources, it also needs comparable conditions or a clear note that the comparison is limited.
Wording That Works
Prefer language like this:
- “In an in vitro biofilm model on stainless steel coupons, the authors reported reduced viable counts after exposure to octenidine hydrochloride under the tested conditions.”
- “The P. aeruginosa adaptation study reported increased tolerance after repeated exposure, with organism-specific genetic and membrane changes.”
- “The MRSA network study did not find a direct association between octenidine exposure and reduced octenidine susceptibility in its isolate set.”
- “Resistance language should be read through the source’s assay, threshold, and organism context.”
Avoid language like this:
- “Octenidine eradicates biofilm infections.”
- “Biofilm results prove wound, catheter, or device outcomes.”
- “Membrane-active antiseptics cannot select for reduced susceptibility.”
- “qac genes prove octenidine resistance.”
- “Antibiotic-resistant organisms are automatically octenidine-resistant.”
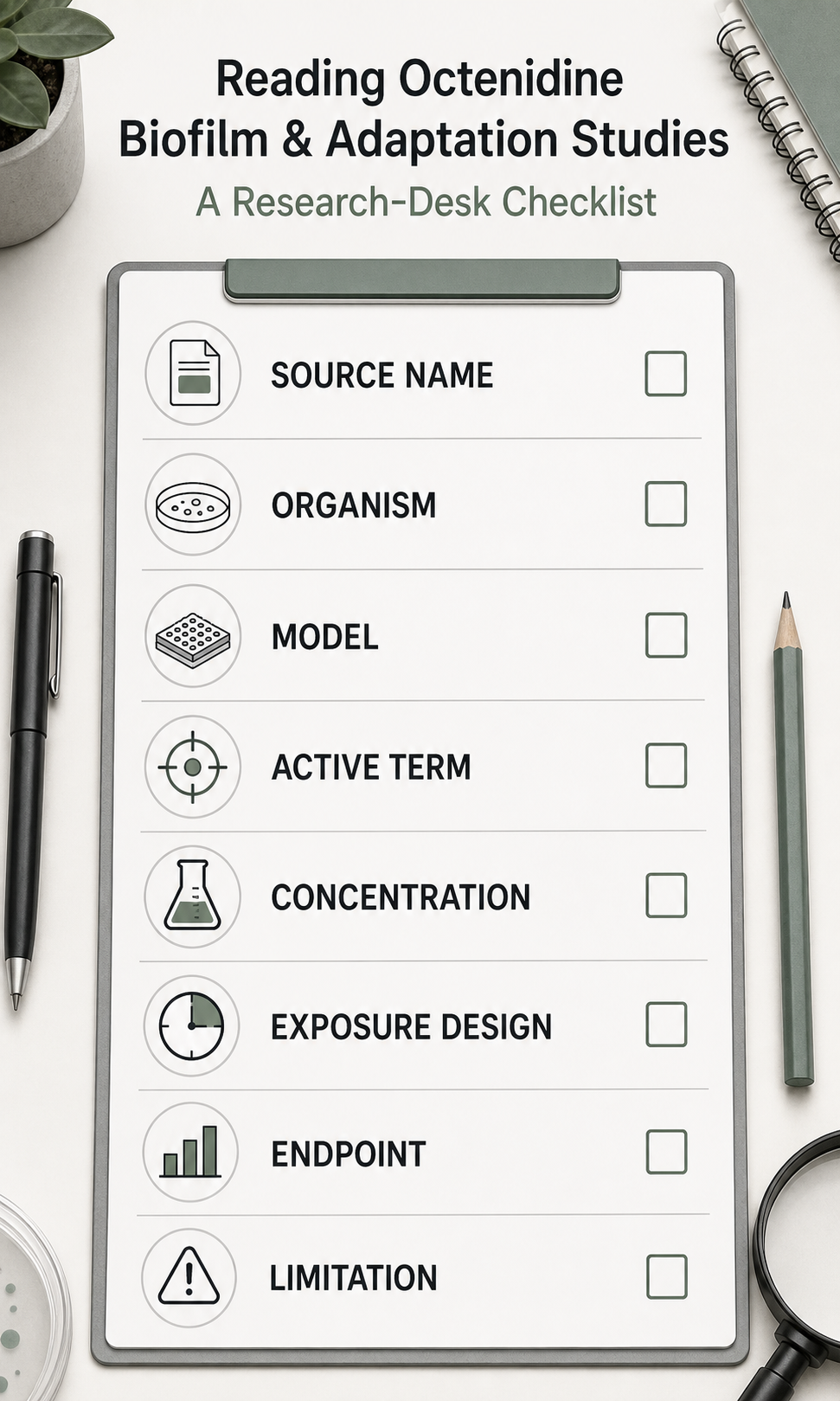
Researcher Claim Checklist
When interpreting a biofilm, tolerance, or resistance statement, check the source against these questions:
- What exact name did the source use: octenidine, octenidine hydrochloride, octenidine dihydrochloride, OCT, or a finished product?
- Was the evidence planktonic, biofilm, mixed culture, simulated clinical setting, observational surveillance, or clinical outcome evidence?
- Which organism, strain, isolate set, or microbial community was tested?
- Was exposure short, repeated, escalating, diluted, or in-use-concentration based?
- Was the endpoint MIC, MBC, survival after contact time, CFU reduction, microscopy, mutation, gene carriage, or association with use?
- Did the source define resistance, tolerance, adaptation, or reduced susceptibility?
- Did the source test antibiotic susceptibility separately, or only antiseptic and biocide susceptibility?
- Could a reader mistake the statement for a patient-care or product-use claim?
If any answer is missing, keep the wording narrower.
Sources And Review
Last reviewed: 2026-05-28. References used here include official identity records, biofilm model studies, Pseudomonas adaptation studies, Staphylococcus reduced-susceptibility studies, and broad disinfectant, antiseptic, and biofilm terminology reviews.
Editorial review is not medical advice, regulatory advice, infection-control advice, or a clinical recommendation.