Octenidine sits in a live research question: can a skin antiseptic reduce a difficult fungal colonizer without flattening the larger ICU skin microbiome or selecting a resistance problem that the original endpoint did not measure?
The short answer is cautious. Recent sources support octenidine as an important candidate for reducing Candida auris burden in ex vivo human skin and in vitro biofilm models. A separate ICU bathing study suggests that daily 0.08% octenidine wash mitts did not measurably disrupt bacterial microbiome structure or increase selected antibiotic resistance genes compared with water-and-soap bathing. Those are related findings, but they are not the same endpoint.
Quick Position
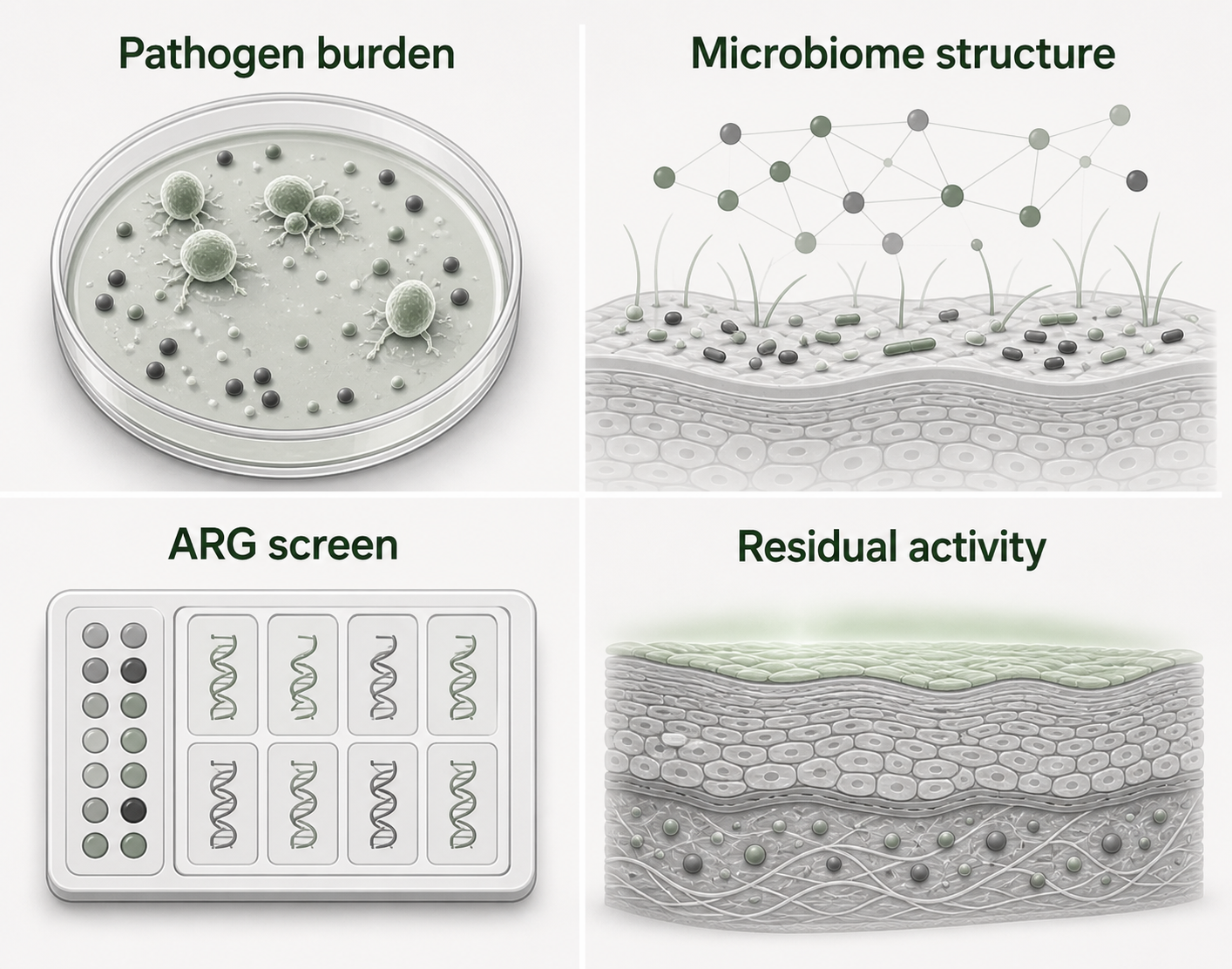
The useful reading move is to keep four endpoints separate:
- C. auris colonization: how much viable fungus remains on or in a skin model after an antiseptic exposure.
- Microbiome structure: whether bacterial communities on ICU skin change in biomass, diversity, site specificity, or taxonomic composition after bathing.
- Resistance-gene screening: whether selected antibiotic resistance genes become more common in sampled skin communities.
- Residual activity: whether antiseptic activity remains measurable on a reconstructed epidermis model after topical exposure.
The sources point in a coherent direction, but not a simple one. Octenidine can look strong against C. auris in a controlled skin model, while whole-skin ICU bathing may show a smaller or different signal against bacterial biomass. A microbiome study can reassure on selected community endpoints without proving fungal decolonization. A residual-activity study can support remanence in a reconstructed epidermis model without proving outbreak control.
That distinction keeps the evidence useful.
Why Candida auris Makes Skin Evidence Harder
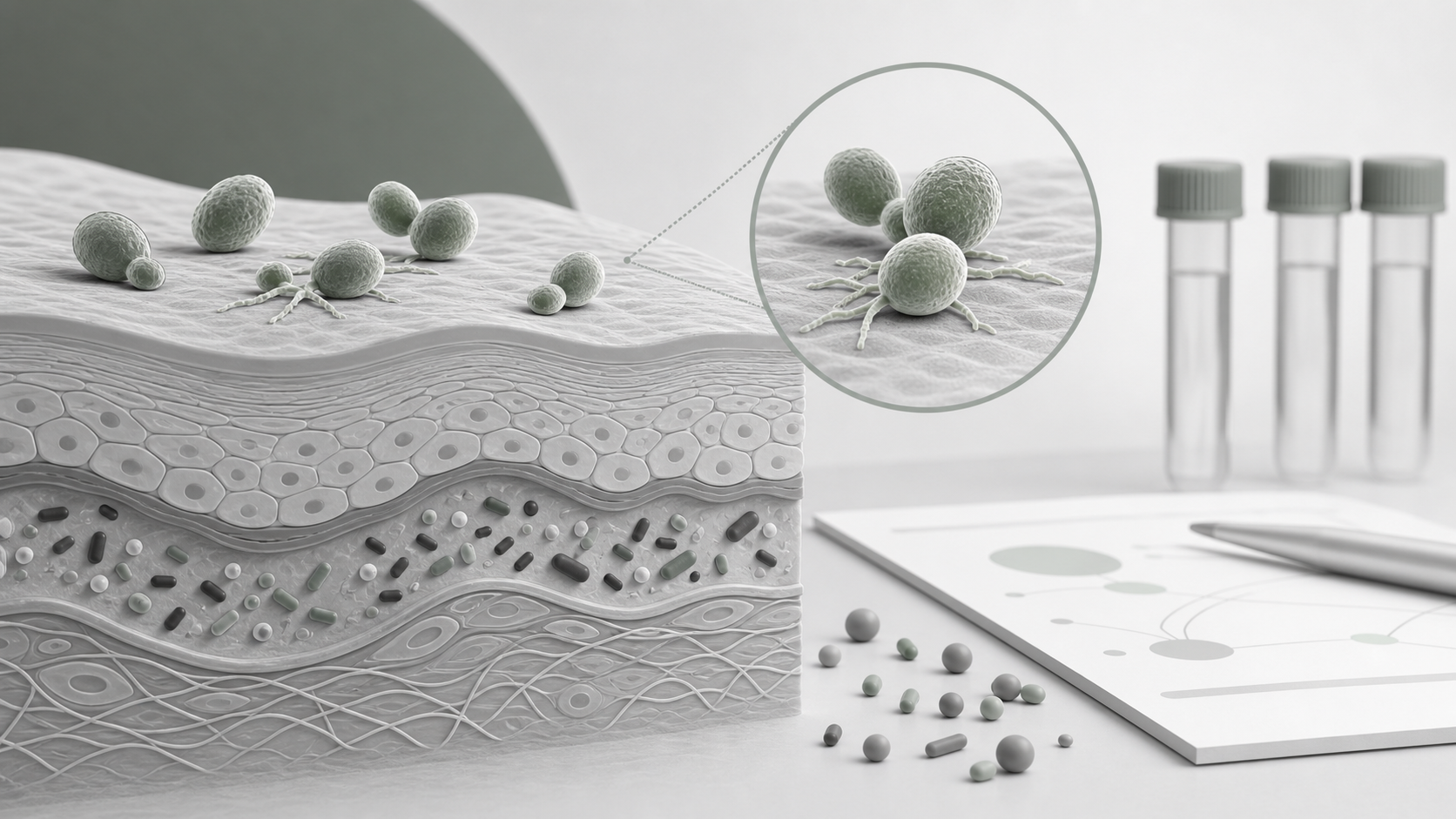
Candida auris is not just another Candida name on a lab list. It is a healthcare-associated fungal pathogen with strong skin tropism, outbreak relevance, environmental persistence, and frequent resistance to systemic antifungals. Skin colonization matters because colonized patients can seed nearby surfaces and because ICU patients often have devices, damaged barriers, antibiotic exposure, and impaired host defenses.
That does not make every decolonization claim valid. It makes the endpoint more important.
For C. auris, a skin antiseptic source should tell the reader what was tested: intact skin or wounded skin, live skin or reconstructed epidermis, planktonic cells or biofilm, wipe or drop application, concentration, contact time, clade or strain, and the method used to count surviving organisms.
What The Candida auris Skin Study Can Support
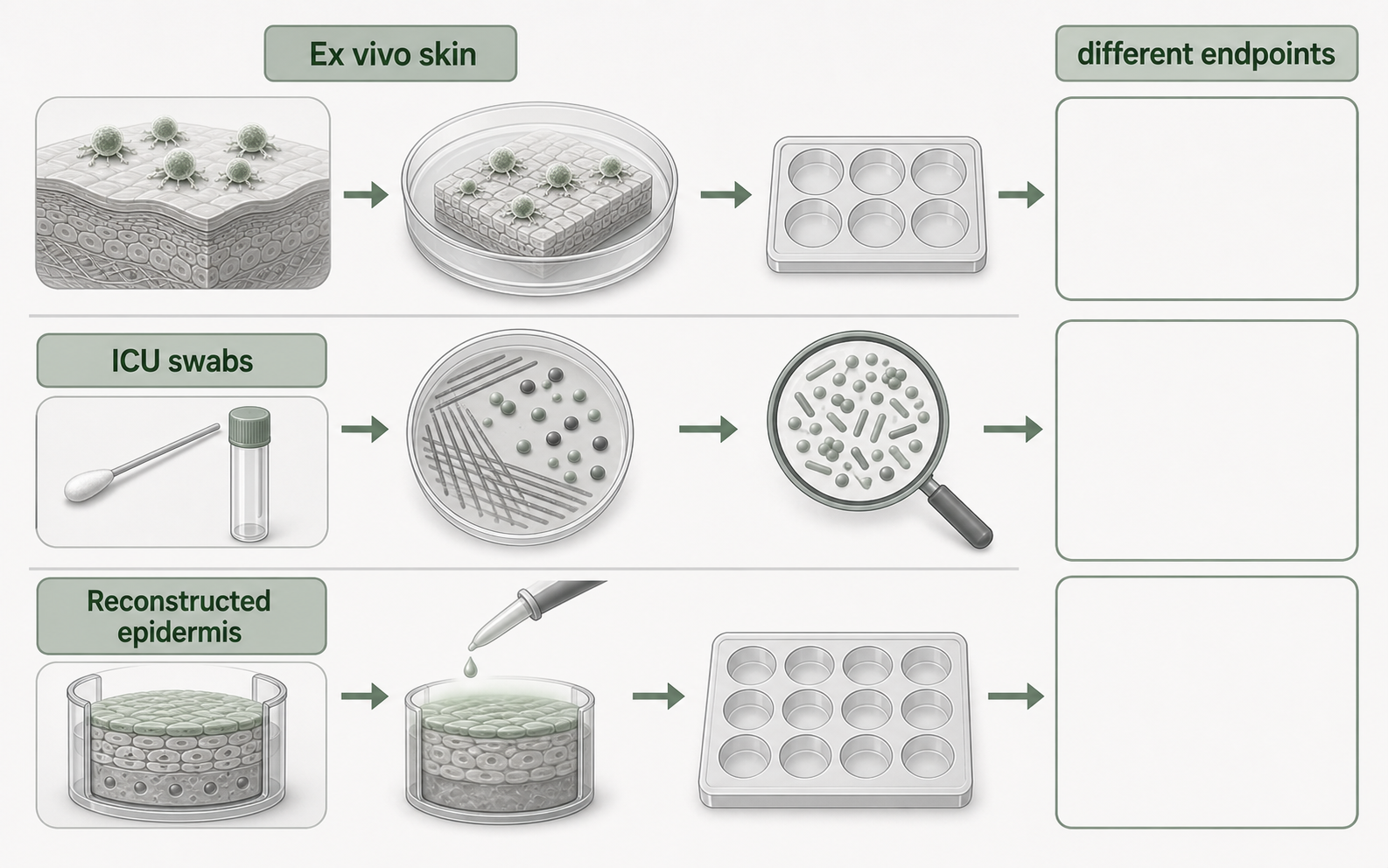
The 2025 Scientific Reports study tested commercial octenidine-based antiseptics against C. auris using ex vivo human skin and in vitro biofilm assays. Fresh human skin from healthy adult donors was used as intact or needled skin. The study applied C. auris to skin biopsies, waited six hours, treated with octenisept, octeniderm, 2% chlorhexidine gluconate, or PBS control, and assessed fungal colonization after 18 hours using histology, microscopy, scanning electron microscopy, and CFU quantification.
That design supports a model-specific statement: octenidine-based products reduced viable C. auris on intact and wounded ex vivo human skin under the tested conditions. The study also tested several C. auris strains from different clades in an in vitro biofilm assay and reported strong antifungal activity after antiseptic treatment.
The result is promising because it uses human skin tissue rather than only a hard-surface or planktonic suspension assay. It also matters that the study explicitly looked at wounded skin, because barrier disruption changes where C. auris can be found in the model.
The limit is just as important. Ex vivo skin is not a living ICU patient. It does not reproduce blood flow, systemic immunity, sweating, repeated patient turning, friction from wash mitts, competing hospital exposures, recolonization, room contamination, or protocol adherence. The paper itself points toward the need for clinical validation of commercial products intended for whole-body decolonization during C. auris outbreaks.
What The ICU Microbiome Bathing Study Can Support
The 2025 Medical Microbiology and Immunology study asked a different question. It used samples from a three-armed cluster randomized decolonization trial and compared water-and-soap bathing with 2% chlorhexidine cloths and 0.08% octenidine wash mitts. The microbiome sub-study included 26 ICU patients and sampled five skin sites at three time points: within 12 hours after ICU admission, before the fifth bathing during ICU stay, and five days after ICU discharge.
The methods were broader than a simple culture count. The authors used culture-based methods, 16S rRNA gene amplicon sequencing, bacterial biomass measurements, and multiplex Taq-Man assays for selected antibiotic resistance genes. The sites included axillary vault, hypothenar palm, gluteal crease, nares, and external auditory canal; the first three were included in bathing protocols, while the nares and external auditory canal were not.
The study found that chlorhexidine bathing led to a sustained reduction of bacterial biomass at different skin sites. Octenidine showed a significant reduction in gluteal-crease bacterial biomass by qPCR, but the culture-based contact plate validation did not confirm an octenidine reduction in the tested axilla and palm sites. Across strategies, the larger bacterial community structures were mostly preserved. The loss of normal skin site specificity seen in ICU patients persisted regardless of bathing method and even after discharge.
For resistance-gene screening, the study detected three genes in the sample set: blaSHV, blaCTX-M1, and mecA. The water-and-soap cohort showed an increase in normalized mecA presence in washed sites at later time points compared with unwashed sites. The chlorhexidine and octenidine cohorts did not show a significant increase in detected ARGs over time. That is reassuring within the gene panel and sample size, but it is not a general proof that antiseptic use cannot select for resistance.
Most importantly for this article, the ICU bathing study was not a C. auris decolonization study. It helps answer whether daily octenidine bathing visibly disturbed bacterial skin microbiome structure or selected the measured ARGs in that cohort. It does not answer whether octenidine reduces C. auris colonization in ICU patients.
Residual Skin Activity Is Another Endpoint
The 2014 Skin Pharmacology and Physiology study tested residual antimicrobial activity after reconstructed human epidermis was exposed for 15 minutes to equimolar chlorhexidine digluconate or octenidine dihydrochloride solutions. The model then assessed activity against Staphylococcus aureus and Pseudomonas aeruginosa.
That source is useful because residual activity is often invoked in antiseptic interpretation. In the model, epidermis-associated antiseptic activity was stronger against S. aureus than against P. aeruginosa. Small amounts of both antiseptics penetrated the stratum corneum, and the authors discussed antimicrobial activity alongside keratinocyte viability.
But this source should not be stretched into a C. auris conclusion. It did not test C. auris. It did not measure ICU microbiome structure. It did not test patient decolonization or transmission. It supports a narrower point: residual antimicrobial activity can be measured on a skin-like model, and the organism, exposure, and tissue model shape the result.
How The Endpoints Fit Together
The tempting shortcut is to say: octenidine reduces C. auris, leaves the microbiome alone, does not select resistance genes, and has residual activity. That sentence is too smooth.
A more accurate synthesis is this:
- The C. auris skin paper supports antifungal activity in ex vivo human skin and in vitro biofilm models under defined product and exposure conditions.
- The ICU bathing paper supports limited conclusions about bacterial biomass, bacterial community structure, site specificity, and selected ARGs during daily bathing with 0.08% octenidine wash mitts.
- The reconstructed epidermis paper supports model-based residual activity after topical exposure, with organism-specific results.
- The 2025 systematic review shows why decolonization and disinfection claims for C. auris remain agent-, concentration-, exposure-, surface-, model-, and setting-dependent.
Read together, the sources make octenidine worth watching in C. auris skin-colonization research. They do not close the clinical question of patient decolonization during an ICU outbreak.
Why Resistance-Gene Language Needs Care
Resistance genes in a skin microbiome study are not the same thing as antiseptic resistance in a target pathogen. In the ICU bathing study, ARG screening focused on selected antibiotic resistance determinants, including mecA and beta-lactamase genes. That is a useful surveillance-style endpoint for the sampled bacterial community.
It is not a direct test of C. auris antifungal resistance. It is not a full resistome analysis. It is not a demonstration that octenidine use has no selection effects under all durations, concentrations, organisms, or hospital conditions.
For source language, “no increase in selected ARGs was detected in this cohort” is much better than “octenidine does not cause resistance.” The first sentence names the endpoint. The second outruns it.
Where The Systematic Review Helps
The 2025 systematic review of environmental disinfection and decolonization for C. auris is useful because it keeps the field from sounding more settled than it is. The review found heterogeneous evidence across disinfectants, antiseptics, ultraviolet approaches, surfaces, concentrations, contact times, and models. It also emphasized that patient decolonization remains challenging and that many promising approaches have been tested mainly outside human clinical decolonization settings.
That is the right background for the octenidine papers. A strong ex vivo or in vitro result is not weak evidence. It is simply evidence for a model question. The next question is whether the same product format, application method, body site, exposure, and patient population show a meaningful effect in clinical practice.
A Useful Claim Template
For a researcher-facing article, octenidine and C. auris claims should keep the endpoint in the sentence:
- “In an ex vivo human skin model, two octenidine-based products reduced C. auris viability on intact and wounded skin under the tested conditions.”
- “In a small ICU microbiome sub-study, 0.08% octenidine wash mitt bathing did not produce a detectable broad shift in bacterial microbiome structure or an increase in the selected ARG panel.”
- “Residual antimicrobial activity has been shown on reconstructed human epidermis against tested bacteria, but that endpoint is not a C. auris decolonization outcome.”
- “Clinical decolonization and outbreak-control claims still need patient-level evidence tied to the exact product, application method, and setting.”
The same template also prevents overreach. If a sentence drops the model, organism, concentration, exposure, or endpoint, it probably needs another pass.
Sources And Review
The cited studies have four roles. The Candida auris skin study supplies the direct octenidine antifungal model evidence. The ICU bathing study supplies microbiome-structure and selected ARG evidence. The reconstructed epidermis paper supplies residual-activity context. The systematic review supplies the broader boundary for C. auris environmental disinfection and decolonization evidence.
Read this page as a research-interpretation brief, not as a decolonization protocol or product-use recommendation. The key publication boundary is the same throughout: ex vivo reduction, selected ARG screening, and residual activity become useful only when the model, organism, formulation, exposure, and endpoint remain visible.