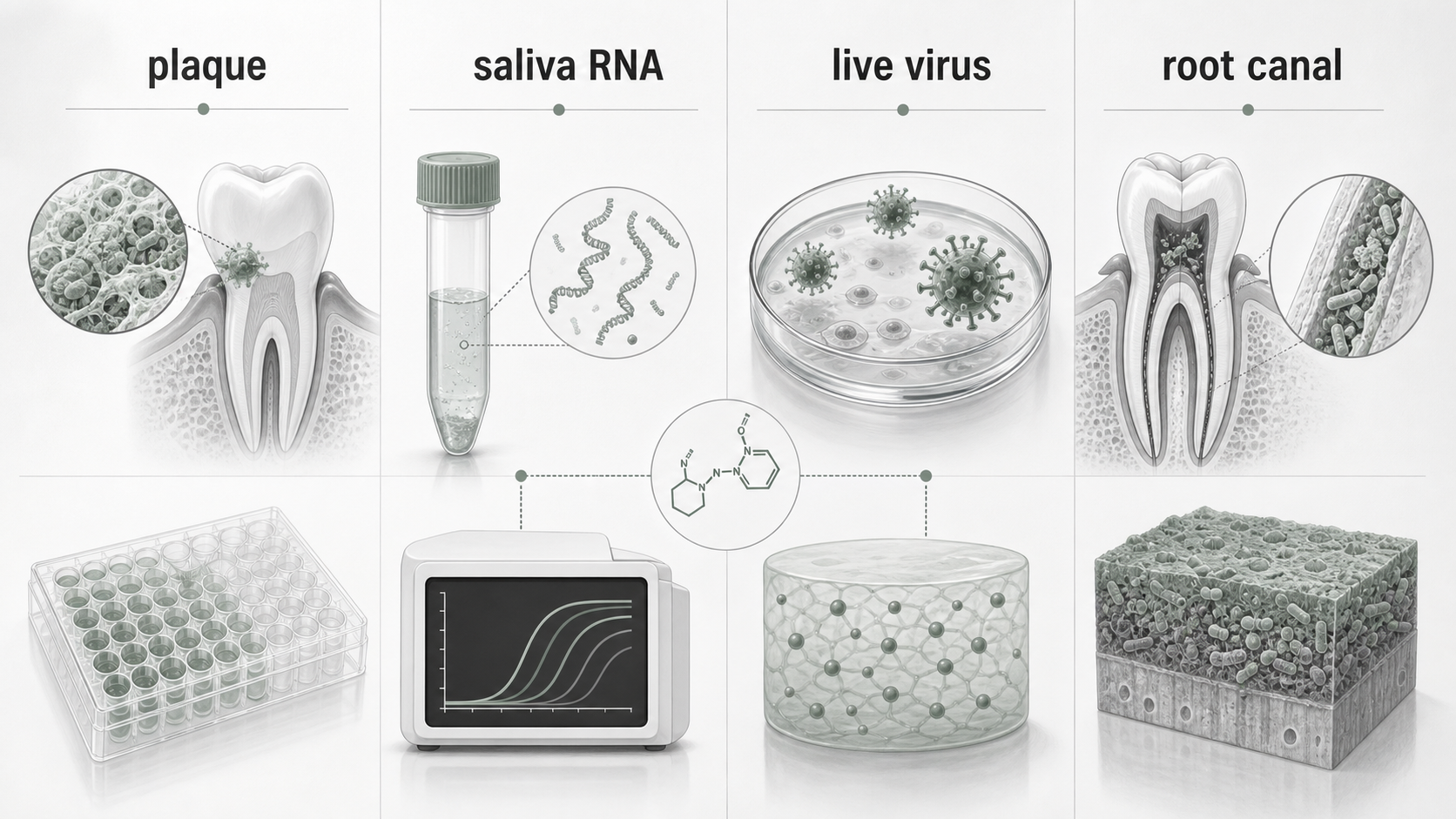
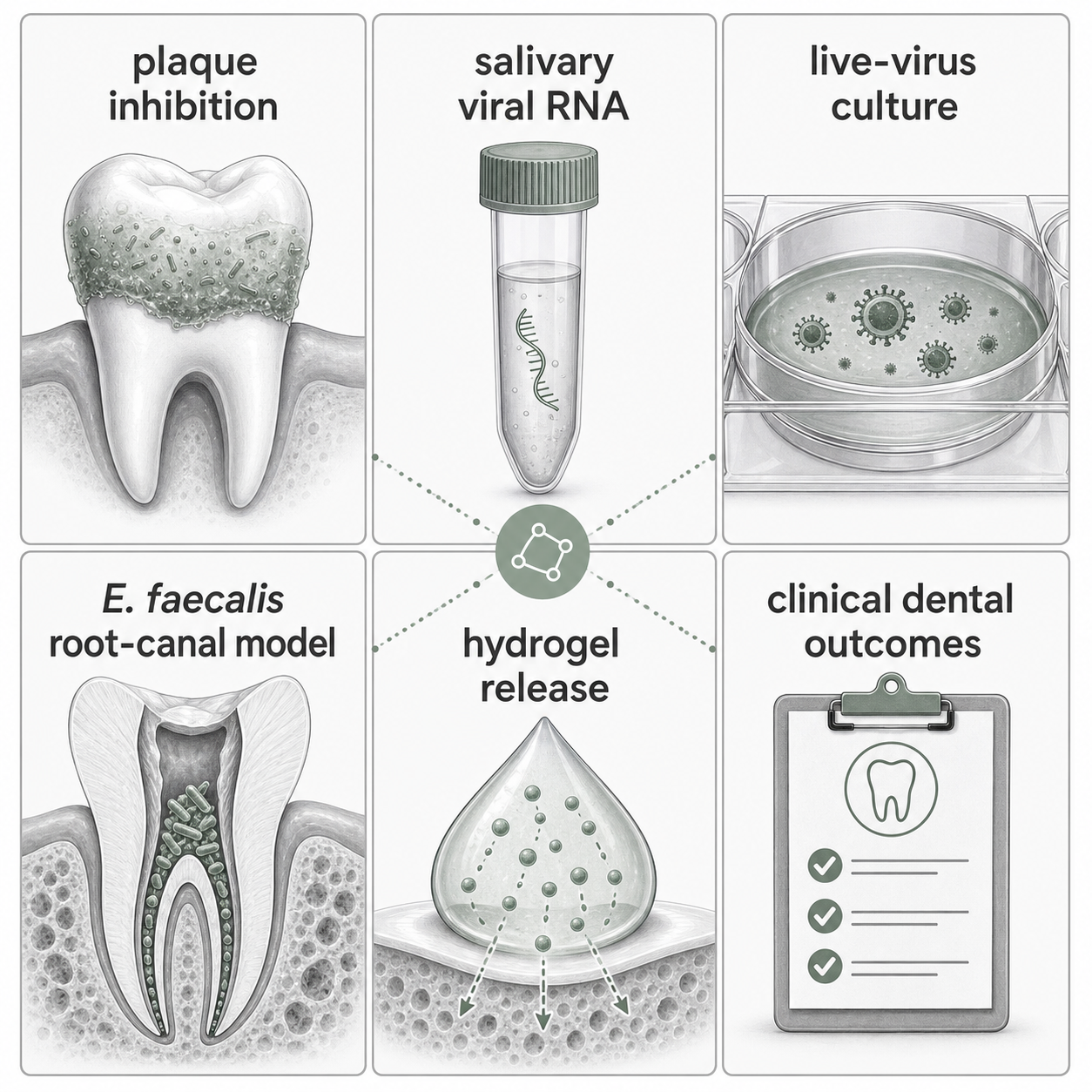
Octenidine oral research is not one evidence bucket. A dental-plaque inhibitor study, a saliva viral-RNA study, a live-virus culture result, an extracted-tooth root-canal biofilm model, and a hydrogel release study can all involve octenidine and still answer different questions.
The useful reading move is simple: keep the formulation, site, model, contact time, organism or virus endpoint, and outcome attached to each claim. That makes the evidence more informative and prevents a laboratory result from becoming a clinical dental conclusion it did not test.
Quick Position
Octenidine has appeared in oral and dental research for several reasons: inhibition of plaque organisms, mouth-rinse effects on SARS-CoV-2 in saliva, virucidal testing across antiseptics, antimicrobial activity in infected root-canal models, and designed release systems for apical-periodontitis research.
Those lines of evidence should not be collapsed. Plaque regrowth is not the same endpoint as salivary viral RNA. Salivary viral RNA is not the same endpoint as infectious virus recovery. Enterococcus faecalis in an extracted root canal is not the same endpoint as clinical success after endodontic treatment. A thermosensitive hydrogel that controls octenidine release is not the same evidence object as a chairside rinse or irrigant.
For a researcher or evidence reviewer, the useful rule is this: oral octenidine evidence is best read by endpoint and model, not by ingredient name alone.
Plaque Research Started With Candidate Selection
The 1984 bispyridinamine paper is useful because it shows early dental-plaque thinking around octenidine as a topical antimicrobial candidate. It compared a series of bispyridinamines for properties relevant to plaque inhibition and identified octenidine among compounds selected for clinical study.
That does not make the paper a modern clinical practice source. It is a candidate-selection and topical antimicrobial source. It belongs in the evidence history because it connects octenidine chemistry to dental-plaque inhibition, but it should not be used as a stand-alone claim that a specific current mouth rinse improves gingivitis, caries risk, periodontal outcomes, or oral infection outcomes.
A later phase 3 plaque-regrowth study of 0.1% octenidine mouthwash in healthy adults is closer to a clinical dental-mouthwash endpoint. Even there, the claim should stay narrow: formulation, population, short regrowth model, comparator, and plaque measurement matter. A plaque-regrowth model can support a plaque-control statement more directly than the 1984 chemistry paper, but it still does not answer root-canal, viral-load, or apical-periodontitis questions.
Viral Load Studies Need The Assay Named
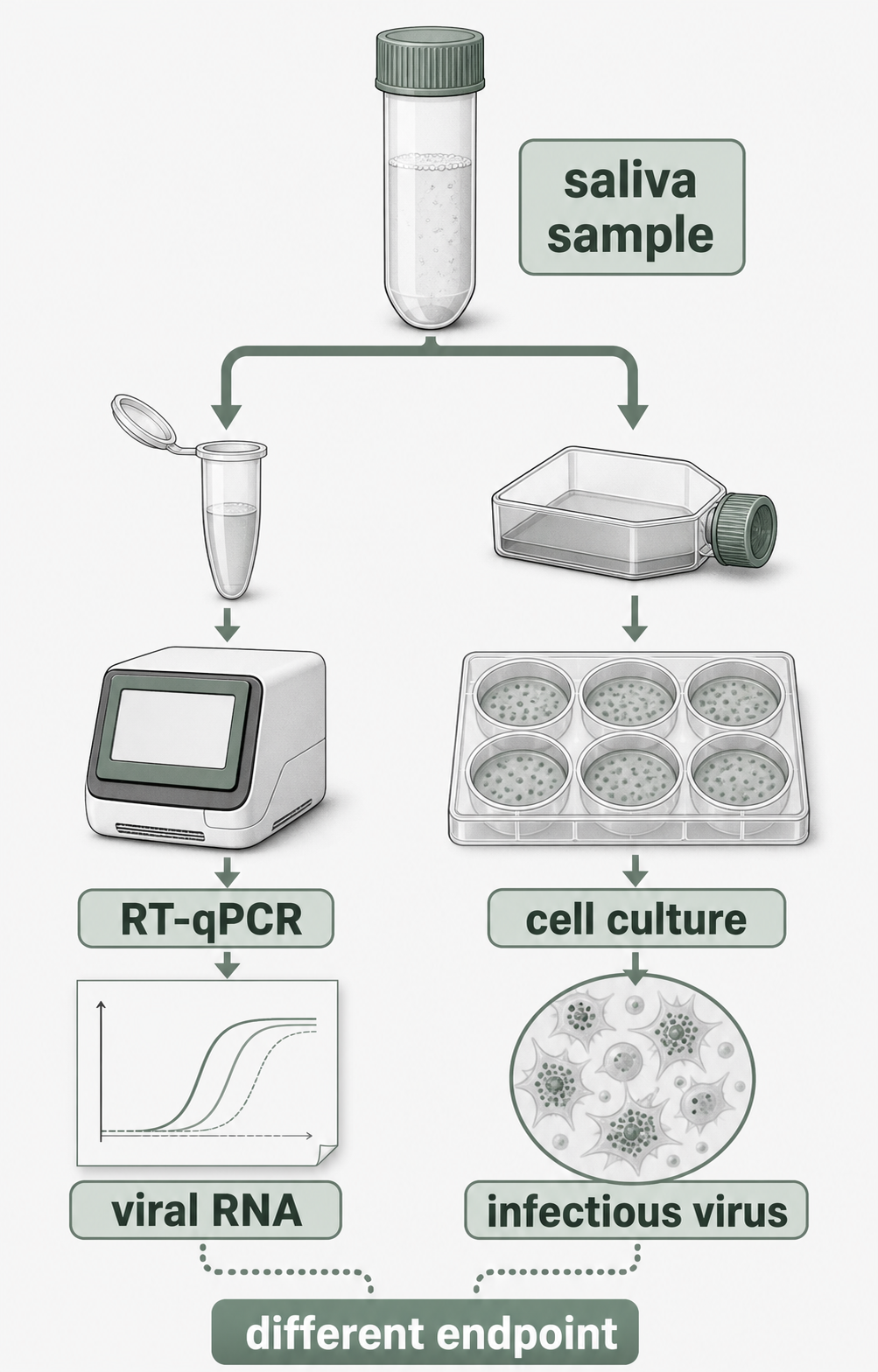
The 2022 oral-rinsing study tested an octenidine-based mouth-rinse setting in people with SARS-CoV-2 infection and measured saliva samples over time. Its key strength is that it did not ask a vague “does octenidine work in the mouth” question. It asked a timed saliva question after rinsing and used molecular detection to follow viral load.
That design matters. A drop in detectable viral RNA shortly after rinsing is a saliva sampling and RT-qPCR endpoint. It can be relevant to transient oral viral-load reduction, but it is not automatically a transmission outcome, a clinical COVID-19 outcome, or a general statement about all mouth rinses.
The same study also included culture work, which is an important separate endpoint. Viral culture asks whether infectious virus can be recovered under the assay conditions. When baseline culture recovery is limited or absent, culture data cannot be read as a direct demonstration that the rinse reduced live infectious virus from a known positive baseline. That is not a flaw in the study; it is the boundary of what the assay showed in that sample set.
The SARS-CoV-2 Review Does Not Make One Ranked Octenidine Answer
The systematic review and Bayesian network meta-analysis on antiseptics against SARS-CoV-2 is useful for another reason: it shows how hard it is to compare oral antiseptics when formulations, concentrations, contact times, and endpoints differ.
The review included multiple antiseptic agents and both in vitro and in vivo evidence. Network ranking was possible only where the evidence network could support it. Octenidine appears in the broader antiseptic evidence set, but sparse or methodologically different data should not be treated as if it produced the same kind of ranked estimate as agents with denser, more connected evidence.
For article wording, this means the review can support a cautious evidence-map claim: oral antiseptic SARS-CoV-2 findings are formulation-specific and assay-specific, and network comparisons depend on how much comparable evidence exists. It should not be used to say that octenidine is clinically superior, inferior, or interchangeable with another antiseptic for dental care.
Root-Canal Biofilm Models Ask A Different Question
Root-canal research shifts the endpoint again. The 2025 in vitro irrigant study tested antimicrobial effects against E. faecalis in root canals, using an infected-root model and comparing irrigants that included EDTA and octenidine dihydrochloride. That is much closer to an endodontic methods question than to a mouth-rinse question.
The practical reading boundary is the model. Extracted teeth, standardized contamination, irrigant contact, sampling method, and culture endpoint all shape the result. If a source reports that an octenidine-containing irrigant performed better than EDTA alone, that is a model-specific antimicrobial finding. It is not, by itself, proof of clinical success, long-term healing, retreatment reduction, or superiority over sodium hypochlorite in practice.
This is especially important because endodontic papers often compare chemically different irrigant strategies. EDTA is commonly discussed for smear-layer or chelation context, while sodium hypochlorite, chlorhexidine, and octenidine-containing formulations may be discussed for antimicrobial activity. A fair comparison has to name which property is being measured.
Hydrogel Release Adds Formulation Engineering
The 2024 thermosensitive hydrogel paper adds another layer: programmed dual release. It studied a delivery system designed to release hydrophilic octenidine hydrochloride and hydrophobic octenidine in different patterns, with biofilm and apical-periodontitis model endpoints.
That source is valuable because it keeps formulation engineering visible. A hydrogel can change exposure time, local retention, burst release, sustained release, and contact with a biofilm model. Those properties are not equivalent to adding the same active substance to a rinse bottle or using an irrigant for a brief final rinse.
The source can support careful language about a designed octenidine delivery system showing antimicrobial and model outcomes under the tested conditions. It should not be rewritten as a patient instruction, a dental-procedure recommendation, or proof that an octenidine hydrogel is clinically established for apical periodontitis.

Dentistry Context Helps, But It Does Not Replace Primary Endpoints
The broader dentistry review on synthetic compounds can help place octenidine alongside other compounds discussed in dental materials, antisepsis, and antimicrobial contexts. It is useful for orientation, terminology, and finding adjacent literature.
For evidence claims, though, the primary study still does the work. A review can say that octenidine is relevant to dental antimicrobial research. It cannot make a root-canal model answer a plaque question, or make a saliva viral-RNA result answer a live-virus transmission question.
How To Write The Claim Without Overreaching
For plaque evidence, name the formulation, plaque model, population, duration, and comparator. “Reduced plaque regrowth in a short healthy-adult model” is different from “improves periodontal disease.”
For SARS-CoV-2 saliva evidence, name the rinse formulation, sampling time, and RT-qPCR endpoint. If culture is discussed, say whether infectious virus was recovered and whether the design supports a before-after culture conclusion.
For virucidal reviews, name whether the finding is in vitro, in vivo, qualitative synthesis, or network comparison. Do not treat qualitative inclusion as a ranked estimate.
For root-canal evidence, name the organism, tooth model, irrigant composition, contact time, sampling method, and endpoint. Keep E. faecalis model results separate from clinical endodontic outcomes.
For hydrogel studies, name the delivery system and release design before naming the antimicrobial result. A dual-release depot is a formulation-engineering result as well as a microbiology result.
What This Evidence Does Not Settle
This evidence set does not settle dental treatment protocols, mouth-rinse substitution choices, chairside infection-control policy, endodontic irrigant selection, or patient self-use decisions. It also does not define a universal oral concentration for octenidine or a universal claim that all octenidine-containing products behave the same way.
The evidence is still useful. It shows that octenidine has been studied across oral biofilm, saliva, virus, and endodontic models. Its value improves when the article keeps those models separate.
Sources And Review
The main sources are the 1984 dental-plaque bispyridinamine paper, the 2022 oral-rinsing SARS-CoV-2 saliva study, the 2025 systematic review and Bayesian network meta-analysis of antiseptics against SARS-CoV-2, the 2024 programmed dual-octenidine hydrogel study, and the 2025 in vitro endodontic irrigant study against E. faecalis. The broader dentistry review and plaque-regrowth study are used as context, not as a reason to merge endpoints.
Editorial review is source review. This article is educational context for reading oral octenidine research, not dental advice, infection-control advice, regulatory advice, or a clinical recommendation.