Octenidine residue, tissue concentration, residual antimicrobial activity, scaffold cytotoxicity, and controlled-release data are related, but they do not answer the same question.
That distinction is the main point of this article. A hand-wound LC-MS/MS study can show whether octenidine is measurable in sampled tissue after disinfection. A reconstructed epidermis study can ask whether a short exposure leaves antimicrobial activity on a tissue model. A scaffold study can ask whether an impregnated matrix is antimicrobial and cytocompatible in vitro. A hydrogel study can ask whether a formulation can release octenidine in a programmed way inside a dental model. Each result is useful. None should be stretched into a general claim that every octenidine product is safe, unsafe, effective, or ineffective in open tissue.
Quick Position
For evidence review, the cleanest reading is to separate five questions:
- Can octenidine be measured in tissue after an exposure?
- Does a treated tissue model retain antimicrobial activity after the original liquid is removed?
- Does the same exposure also affect mammalian-cell viability?
- Does a scaffold or hydrogel change delivery, persistence, and local concentration?
- Is the analytical method sensitive and specific enough for the matrix being tested?
Those questions sit next to each other, not inside one another. A measurable residue does not automatically mean a harmful concentration. Residual antimicrobial activity does not automatically mean clinical benefit. Cytotoxicity in a fibroblast or reconstructed epidermis assay does not automatically predict wound healing. A release system can make a formulation more interesting while also making the evidence harder to translate.
Why These Models Get Confused
Octenidine is often discussed as a persistent, membrane-active antiseptic. That broad description is useful, but it can hide the model. Persistence can mean detectable compound in tissue, residual activity on reconstructed epidermis, drug release from a hydrogel, or retained antimicrobial effect from an impregnated scaffold.
Those are not just different ways of saying the same thing. They use different matrices, exposure times, endpoints, organisms, and mammalian-cell systems. A reader who keeps only the word “residual” may miss what was actually measured.
The practical review move is simple: keep the sample, method, endpoint, and limitation in the same paragraph.
Measured Tissue Concentration Answers A Narrow Question
The International Wound Journal hand-wound study sampled subcutaneous tissue from patients with open hand lacerations before and after surgical disinfection with Octenisept, a product containing octenidine and phenoxyethanol. The authors used ultra-high-performance liquid chromatography coupled to tandem mass spectrometry and reported octenidine detection after disinfection in 16 of 20 tissue samples. They described a lower limit of quantification of 10 pg/mL/mg, with estimated mean octenidine concentration below that threshold before disinfection and a quantifiable mean after disinfection.
That study is important because it turns a residue question into a measurement question. It does not merely infer that octenidine contacts open tissue; it measures octenidine in sampled tissue after a defined disinfection event.
The study should still be read narrowly. The sample was hand-wound subcutaneous tissue, the product was a specific octenidine-phenoxyethanol formulation, and the endpoint was tissue concentration by LC-MS/MS. The result does not establish a universal tissue concentration for all wounds, all application techniques, all formulations, all sampling depths, or all time points after exposure.
The study also sits in a safety-sensitive context. The authors discuss toxic reactions reported after pressurized flushing or poorly drained wound pockets with octenidine-containing disinfectants. That does not make the concentration result a clinical toxicity threshold. It does make the exposure route and application method part of the evidence.
Residual Activity Is Not The Same As Tissue Concentration
The reconstructed human epidermis study asked a different question. It exposed reconstructed human epidermis to equimolar solutions of chlorhexidine digluconate or octenidine dihydrochloride for 15 minutes, then evaluated residual antimicrobial activity against Staphylococcus aureus and Pseudomonas aeruginosa. The PubMed abstract reports stronger residual activity against S. aureus than against P. aeruginosa, with S. aureus not detected after 24 hours of contact and about a 2 log10 reduction for P. aeruginosa at the same time point.
That paper also reported that small amounts of both agents can penetrate the stratum corneum in the model. It included a mammalian-cell signal: keratinocyte viability was reduced to 65-75% of untreated reconstructed epidermis control after 24 hours in the presence of test microorganisms. The authors judged octenidine more favorable than chlorhexidine when considering antimicrobial activity and cytotoxic effect in that model.
The useful insight is not “octenidine persists” by itself. The useful insight is that a short topical exposure in a reconstructed epidermis model can leave enough associated antiseptic to affect later bacterial contact, while the same model also records reduced keratinocyte viability. Activity and cytocompatibility are measured together, but they are still model outcomes.
Scaffold Models Add Another Layer
The 2025 acellular dermal matrix study tested impregnated human acellular dermal substitutes in in vitro burn-wound models against multidrug-resistant Pseudomonas aeruginosa and Acinetobacter baumannii. Seven agents were compared, including an Octenilin solution identified in the paper as octenidine dihydrochloride, povidone-iodine, polyhexamethylene biguanide, hypochlorous acid/sodium hypochlorite, acetic acid, colistin, and vancomycin.
This is not a residue study. It is a scaffold-plus-antimicrobial study. The acellular dermal matrix is part of the test system, and the paper asks whether impregnation gives the matrix antimicrobial activity while remaining compatible with fibroblast cells.
The study’s results were mixed across organism form and endpoint. The authors reported strong performance for 1% acetic acid across planktonic and biofilm conditions and high fibroblast viability in their assay. The octenidine-containing Octenilin condition performed differently by organism and model: it was strong against planktonic A. baumannii in the table, showed slight or no activity in the biofilm conditions described, and was associated with cytotoxicity in the NIH 3T3 fibroblast assay.
That pattern is a useful warning for evidence reviewers. A scaffold can alter exposure geometry, retention, dilution, cell contact, and antimicrobial availability. It is possible for the same agent category to look different in planktonic bacteria, 24-hour biofilm, and fibroblast viability endpoints. Reporting only “worked” or “did not work” loses the study.
Release Systems Ask A Formulation Question
The thermosensitive hydrogel paper moves the question again. It describes a composite hydrogel intended for intracanal use in an apical periodontitis research setting. The formulation used hydrophilic octenidine dihydrochloride for burst release and hydrophobic octenidine loaded in PECT nanoparticles for slower sustained release, with calcium hydroxide added to create an alkaline environment.
The study included material characterization, release testing, root-canal models, multispecies biofilm work, and a rat apical periodontitis model. The authors reported short-term and longer antimicrobial effects and described the hydrogel as easier to remove than calcium hydroxide paste in their model.
This is valuable formulation evidence, but it should not be flattened into a claim about ordinary octenidine exposure. A programmed release system changes local concentration over time by design. It also changes the comparator question: calcium hydroxide paste, chlorhexidine gel, blank hydrogel, alkaline hydrogel, octenidine-loaded hydrogel, and dual octenidine-plus-alkaline hydrogel are not interchangeable exposures.
For a researcher brief, the conservative wording is that the hydrogel paper studies a dual-release octenidine delivery strategy in dental biofilm and apical periodontitis models. It does not establish general wound safety, general open-tissue compatibility, or clinical instructions for octenidine products.
What Hydrogel Evidence Can Carry
Hydrogel evidence is strongest when it is used for the formulation question it actually asks: how a carrier changes octenidine availability over time. In the thermosensitive hydrogel paper, the important variables are not just “octenidine present” or “hydrogel present.” They include hydrophilic octenidine dihydrochloride for earlier release, hydrophobic octenidine in nanoparticles for slower release, the alkaline calcium hydroxide environment, gel behavior, removal, biofilm endpoints, and the model used to test the system.
That makes the paper useful for a precise release-system claim: a designed carrier can create a different exposure curve from a rinse, solution, scaffold impregnation, or tissue-residue scenario. It should not be used as a generic claim that hydrogels make octenidine safer, more effective, or clinically suitable. The hydrogel is part of the intervention, not a neutral container.
A good release-system sentence names three things together: carrier design, measured release or exposure window, and the endpoint tested. For example: “In this thermosensitive dental model, a dual-octenidine hydrogel combined early and sustained release with biofilm and apical-periodontitis endpoints.” That sentence is narrower, and more useful, than “octenidine hydrogels treat biofilms.”
Analytical Limits Decide What “Detected” Means
Residue and concentration claims stand or fall on analytical method details. In the hand-wound paper, LC-MS/MS mattered because the study was measuring very small amounts of octenidine in tissue samples. The lower limit of quantification mattered because values below that threshold could be discussed only with care.
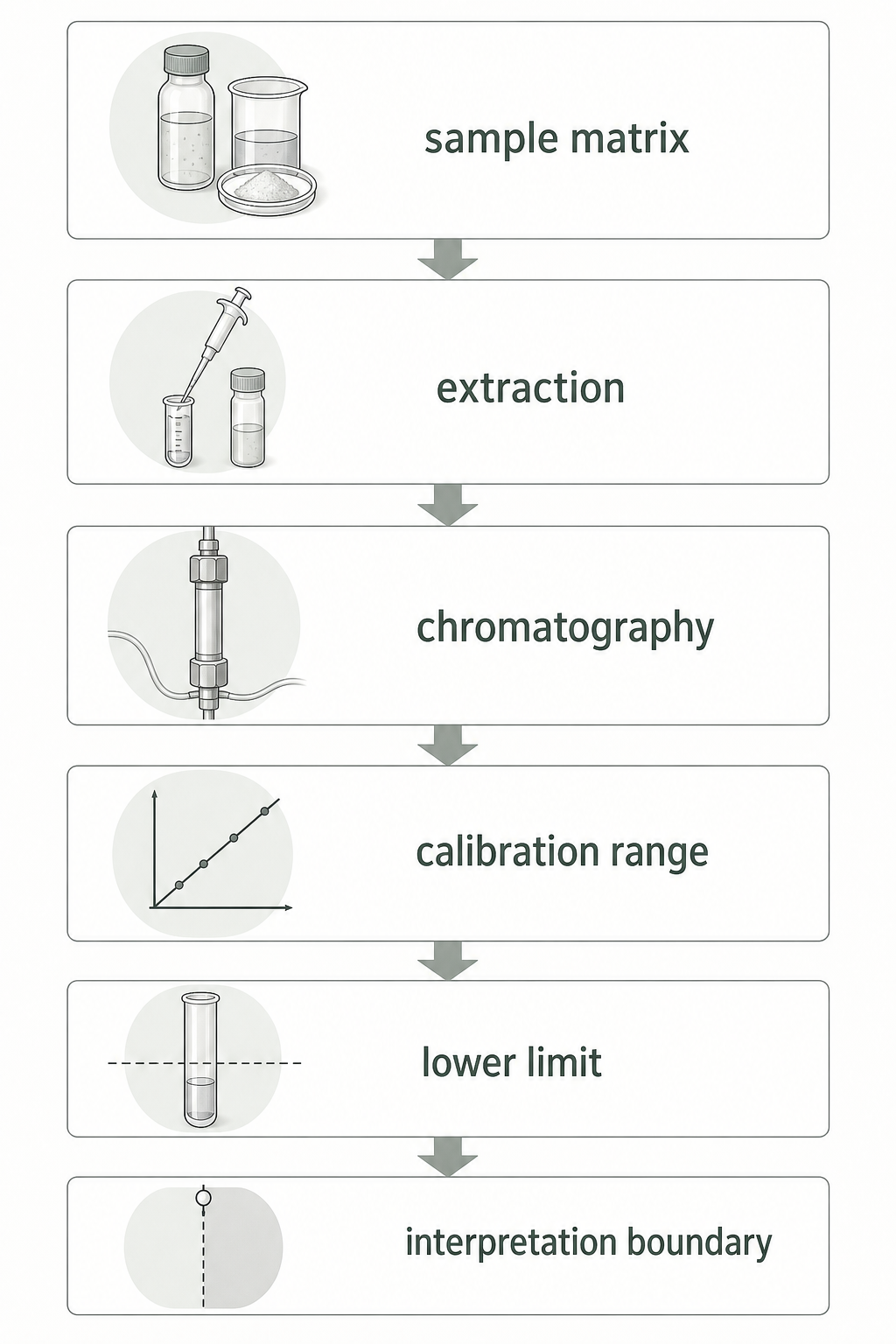
The 2026 RSC Advances paper is useful here because it shows the same broader point in a formulation-quality context. It describes a green RP-HPLC method for simultaneous determination of octenidine dihydrochloride and phenoxyethanol in antiseptic formulations. The method used an isocratic run of about 8 minutes, reported linear ranges of 0.5-3.0 micrograms/mL for octenidine dihydrochloride and 3.0-50.0 micrograms/mL for phenoxyethanol, and listed an octenidine limit of detection of 0.15 micrograms/mL and limit of quantification of 0.5 micrograms/mL.
That formulation assay does not replace LC-MS/MS tissue measurement. It has a different matrix, purpose, sensitivity range, and validation setting. Its value for this article is conceptual: analytical claims are method claims. A number is meaningful only with the matrix, calibration range, specificity, recovery, and quantification limit attached.
HPLC And LC-MS/MS Are Not Interchangeable Proof
HPLC and LC-MS/MS can both support octenidine measurement, but they should not be cited as if they answer the same evidence question. A formulation RP-HPLC assay asks whether octenidine dihydrochloride and phenoxyethanol can be separated and quantified in the tested antiseptic formulation matrix. A tissue LC-MS/MS assay asks whether octenidine can be extracted from biological tissue samples and detected or quantified at the method’s stated limits.
The difference matters when a result is near the method boundary. “Detected” is not the same as “quantified.” “Below the lower limit of quantification” is not the same as absent. A validated range for an antiseptic formulation is not automatically a validated range for subcutaneous tissue, reconstructed epidermis, wound fluid, dentine, scaffold material, or hydrogel samples.
Analytical wording should therefore include the method, matrix, analyte, sample preparation, calibration or validation range, and lower limit of quantification when the source provides them. It should avoid turning a measurement method into a biological conclusion. HPLC can support formulation content. LC-MS/MS can support a tissue-concentration statement. Neither method, by itself, proves antimicrobial activity, cytocompatibility, clinical benefit, or a safe or toxic threshold.
A Practical Reading Frame
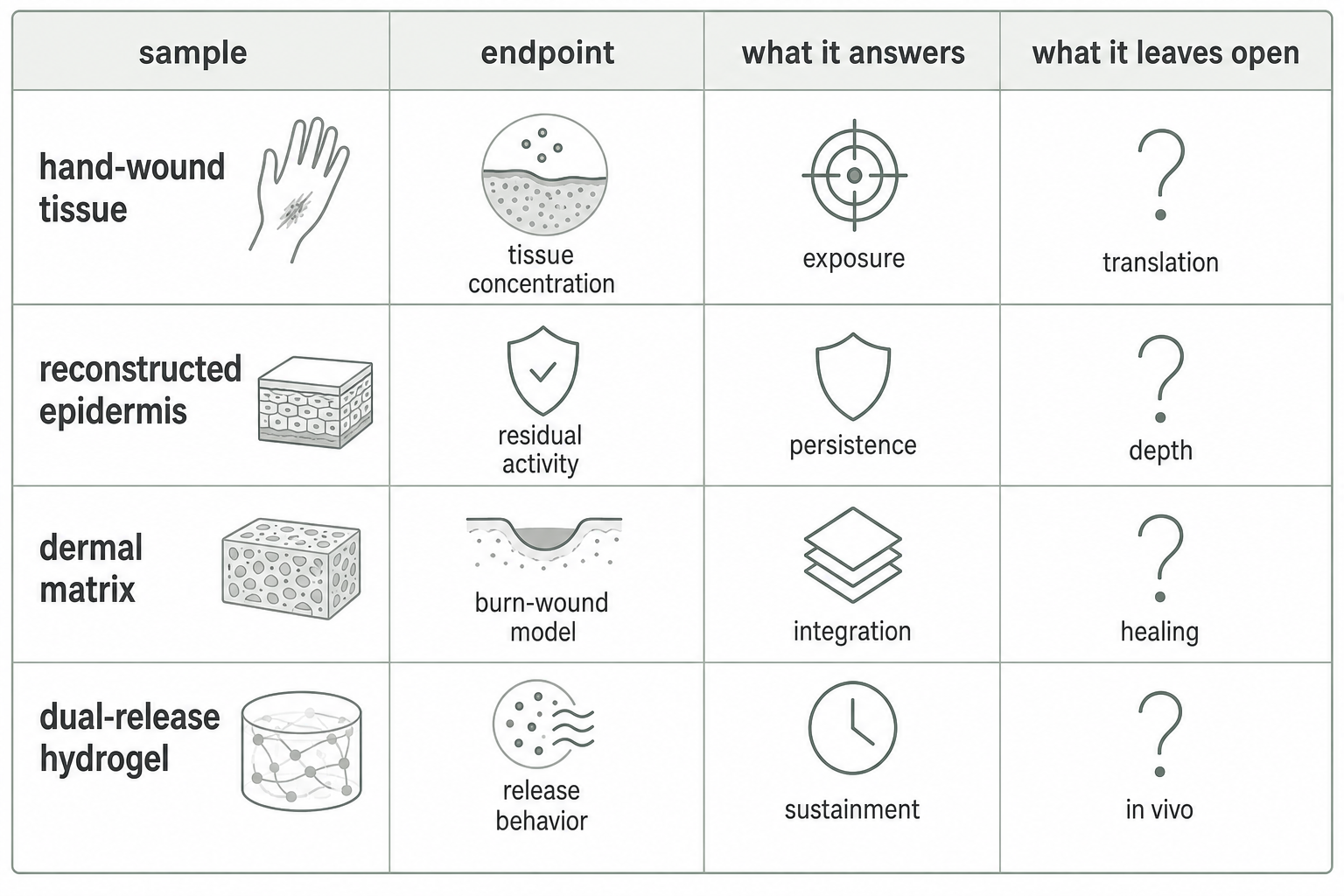
When reviewing an octenidine residue or cytocompatibility source, start with the object in the experiment:
- Tissue sample: asks what can be measured in sampled tissue after a defined exposure.
- Reconstructed epidermis: asks what remains active on or in a skin-like model and how that model’s cells respond.
- Acellular dermal matrix: asks how an impregnated scaffold performs against organisms and with fibroblast compatibility.
- Hydrogel or depot: asks how a formulation controls release, persistence, removal, and local antimicrobial exposure.
- RP-HPLC formulation method: asks whether an analytical procedure can separate and quantify the active and co-ingredient in the tested formulation matrix.
- LC-MS/MS tissue method: asks whether the analyte can be extracted, detected, and quantified in the sampled tissue matrix.
Then attach the endpoint. Antimicrobial activity, viable bacterial count, biofilm disruption, keratinocyte viability, fibroblast viability, concentration, release curve, and quantification limit do not substitute for one another.
The best one-sentence summary for this evidence set is: octenidine can be measurable after certain open-tissue exposures, can show residual antimicrobial activity in reconstructed tissue models, can be delivered by designed release systems, and can perform very differently when placed into scaffold cytocompatibility models.
What This Evidence Does Not Settle
These sources do not settle product directions, clinical wound-care protocols, burn treatment choices, dental treatment instructions, or substitution decisions between antiseptics. They also do not define a universal safe tissue concentration or a universal toxic concentration for octenidine.
That is not a weakness of the papers. It is the boundary of the questions they asked. Keeping that boundary visible makes the evidence more useful, not less.
Sources And Review
The main sources are the 2024 International Wound Journal LC-MS/MS hand-wound concentration study, the 2014 reconstructed human epidermis residual-activity study, the 2025 acellular dermal matrix burn-wound model study, the 2024 dual-octenidine thermosensitive hydrogel study, and the 2026 RSC Advances RP-HPLC paper. The HPLC paper is used for analytical-method context, not as evidence for tissue concentration or clinical safety. Last reviewed: 2026-05-28.
Read this page as a model-interpretation brief. The exact product names, concentrations, matrices, sample counts, quantification limits, and cytocompatibility endpoints are part of the claim. That boundary matters because the article discusses open wounds, burn-wound models, scaffold contact, dental root-canal models, and tissue concentration.