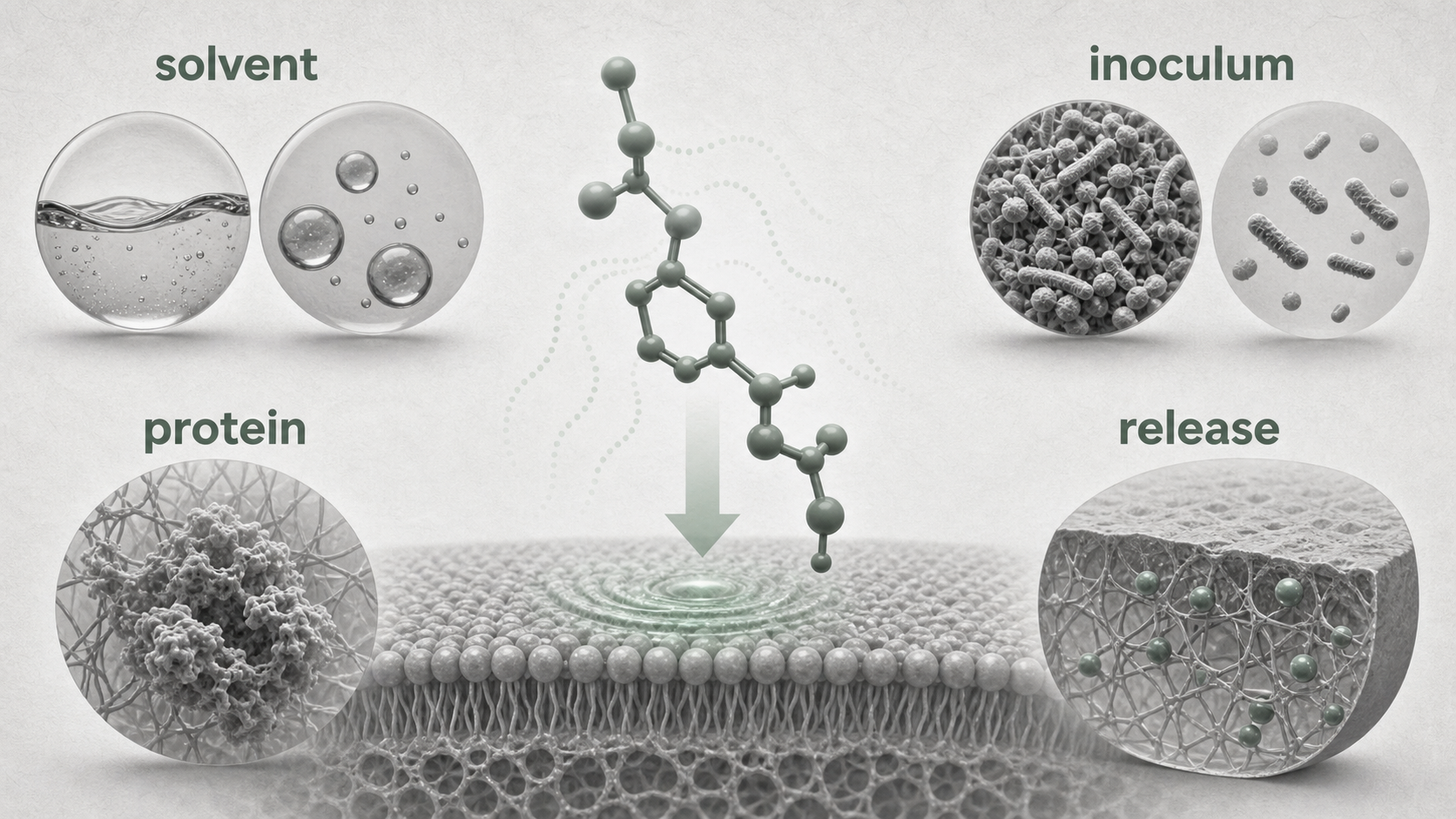
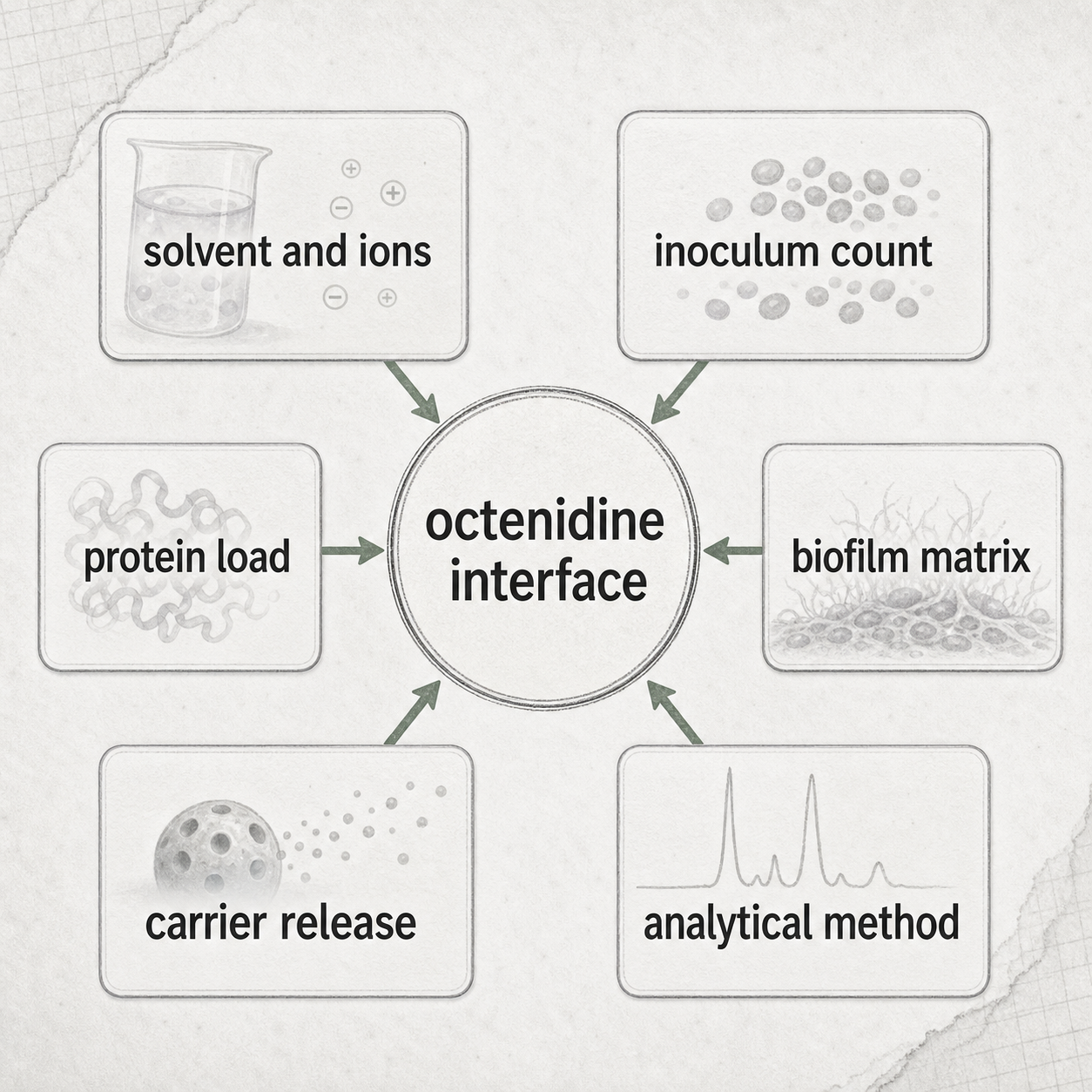
Octenidine results often change because the assay changes the chemical interface. The same active name can meet a different solvent, ion background, inoculum size, protein load, biofilm matrix, carrier-release profile, or measurement method. That changes how much octenidine is freely available, how much reaches cells, and what the endpoint is actually measuring.
For researchers, the practical rule is simple: do not compare octenidine results by nominal concentration alone. Compare the interface.
Quick Position
Octenidine is usually discussed as a cationic, membrane-active antiseptic. That description is useful, but it is not enough to interpret a result. A membrane-active compound can be shaped by the fluid it is dissolved in, the number of cells competing for it, the material surfaces in the assay, organic matter, biofilm structure, and the release system that delivers it.
The 2022 experimental-setup paper makes this visible with Escherichia coli. In that study, octenidine dissolved in water inhibited a standard inoculum at a lower concentration than octenidine dissolved in phosphate-buffered saline or Hepes buffer. Higher bacterial cell counts required higher inhibitory concentrations. Different methods for estimating cell count also changed the apparent result, especially at low octenidine concentrations.
That does not mean every result is unreliable. It means every result has a boundary.
Solvent Is Not Background Noise
Solvent and buffer are easy to treat as neutral parts of a protocol. For octenidine, they can be part of the result.
In the 2022 E. coli study, the authors dissolved octenidine in water, PBS, or Hepes buffer and then measured growth over 20 hours. At an initial bacterial concentration of about 1 x 106 CFU/mL, octenidine in water prevented visible growth at 1 mg/L, while PBS and Hepes required higher concentrations in that experiment. When the inoculum increased up to 2.5 x 108 CFU/mL, the total inhibitory concentration also increased.
The important point is not that one buffer is universally “better.” The point is that ions, buffer composition, possible aggregation, media components, and surface binding can change the amount of octenidine available at the cell envelope. A methods section that says only “octenidine was added” is missing the part that may explain the result.
Inoculum Changes The Dose Per Cell
Octenidine concentration is usually reported as a concentration in the well, tube, canal, or formulation. Cells experience something closer to available molecules per cell surface area.
The 2022 study estimated that bacterial killing required a high coverage of the bacterial surface and that roughly 107 to 108 octenidine molecules were associated with each E. coli cell in its model. The same paper showed that cell-count methods can differ meaningfully. Optical-density estimates, colony counts, and total-cell staining do not necessarily give the same starting inoculum.
This matters most near the threshold. A culture that grows at a low octenidine concentration may reflect reduced susceptibility, but it may also reflect too many cells, too little freely available compound, or an inoculum estimate that shifted the dose-per-cell ratio.
Protein, Organic Matter, And Surfaces Can Sequester The Active
Octenidine’s cationic and amphipathic character is part of its antimicrobial behavior, but it also means the compound can interact with assay materials that are not cells. Growth media, protein, cell debris, plastic or glass surfaces, and biofilm matrix can all compete for the same active.
The 2022 paper explicitly discusses sequestration by growth media or assay plates as one reason low-concentration in vitro results can be hard to compare. Historical microbicidal work from 1985 measured organism killing and skin-degerming activity under its own concentration, exposure, formulation, and extraction conditions. Those experiments are useful historical evidence, but they are not interchangeable with modern buffer-controlled microdilution, biofilm, endodontic, or formulation-release designs.
Protein is especially important in biofilm and wound-like reasoning. It may be present as serum, dentine debris, tissue fluid, collagen-rich matrix, or another organic load. When protein is present, the assay is no longer asking only whether octenidine can act on a planktonic cell. It is asking how the active partitions across cells, proteins, surfaces, and matrix during the exposure window.
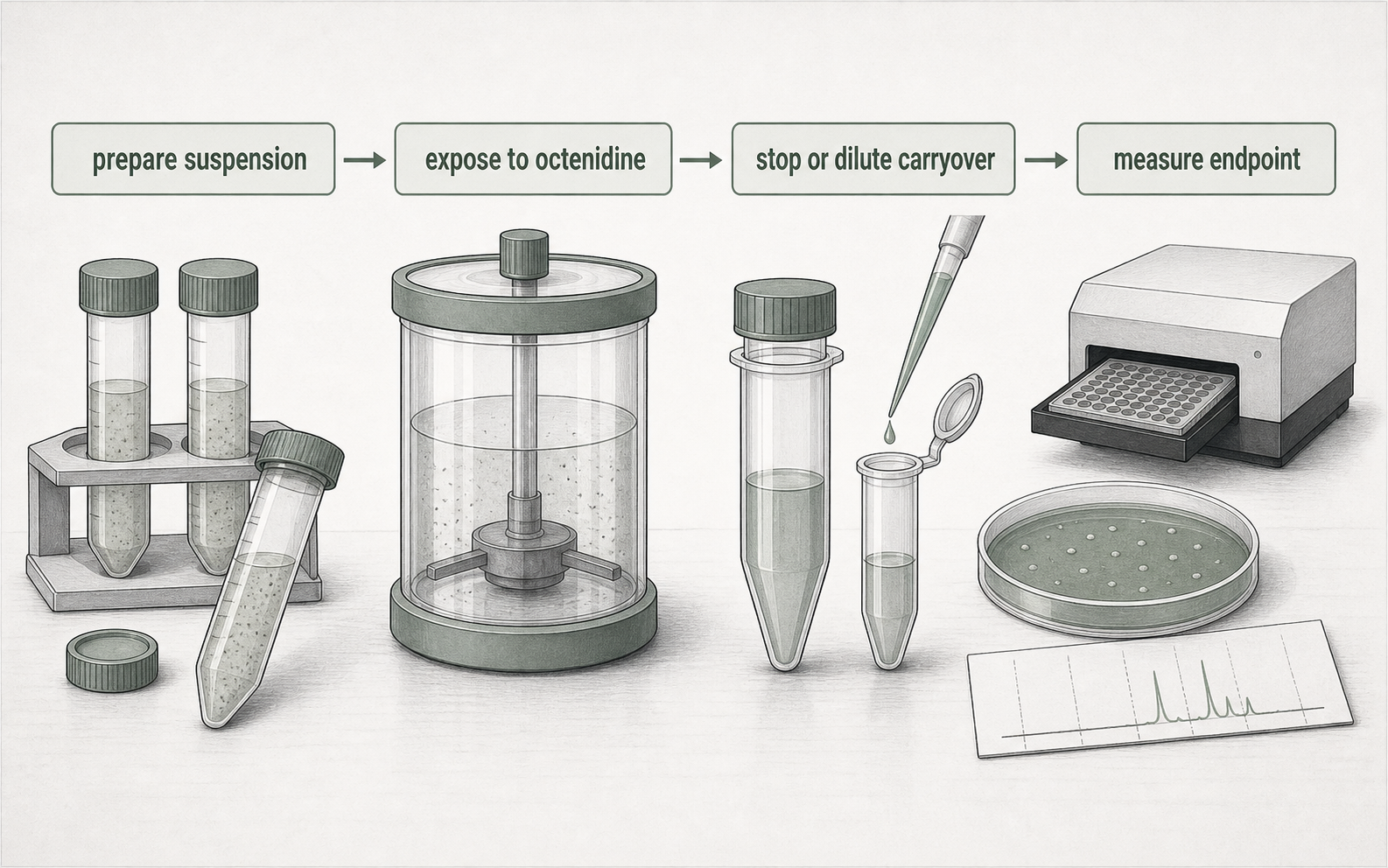
MIC, MBC, And Contact-Time Endpoints Need Different Wording
MIC-style endpoints ask whether visible growth or measured growth is inhibited under a defined incubation system. MBC-style endpoints ask whether viable organisms can be recovered after exposure, neutralization or dilution, and subculture under the method used. Contact-time kill studies ask what happens after a stated exposure window. Those endpoints are related, but they are not synonyms.
For octenidine, the distinction matters because the compound can interact with cells, protein, surfaces, and assay materials. If carryover is not stopped or diluted adequately, an active residue can keep acting during recovery. If the inoculum is higher, the same nominal concentration can mean a lower available amount per cell. If the endpoint is a 20-hour growth curve, it cannot be read like a 1-minute, 5-minute, or 24-hour contact test.
A higher MIC or MBC can support a statement about reduced susceptibility under that method. It does not, by itself, define clinical resistance, product failure, or antibiotic cross-resistance. A cleaner sentence names the endpoint: “the MIC increased in this solvent and inoculum system,” “the MBC changed after repeated exposure,” or “the CFU recovery differed after neutralized dentine-chip sampling.” That wording keeps the result useful without making the assay carry more than it measured.
Biofilm Results Depend On Matrix And Model Geometry
Biofilm assays add another interface: the matrix itself.
An endodontic result may use extracted human teeth, dentinal tubules, a single Enterococcus faecalis strain, a multispecies root-canal biofilm, irrigation with a side-vented needle, dentine chips, blood agar culture, confocal microscopy, scanning electron microscopy, or an animal apical-periodontitis model. Those designs answer different questions.
The 2025 endodontic irrigant study tested 84 extracted single-rooted human teeth divided into seven groups. The Octenisolv group used an experimental irrigant containing 15% EDTA and 0.1% octenidine dihydrochloride. The authors contaminated prepared canals with E. faecalis, incubated them for 7 days, irrigated for 1.5 minutes, applied neutralizers, collected dentine chips, and counted CFU after incubation on blood agar. In that design, 2% sodium hypochlorite produced no bacterial growth, while Octenisolv, Endoxal, and Endosal had relatively good antimicrobial activity and required further clinical study.
That result is not simply “octenidine versus sodium hypochlorite.” It is a final-rinse protocol in a prepared tooth model, with EDTA, a defined contact time, neutralization, dentine sampling, and a culture endpoint.
Release Design Changes The Exposure Curve
A formulation can change results even when the active is familiar. The key variable is not only total octenidine loaded into the system; it is the local concentration over time.
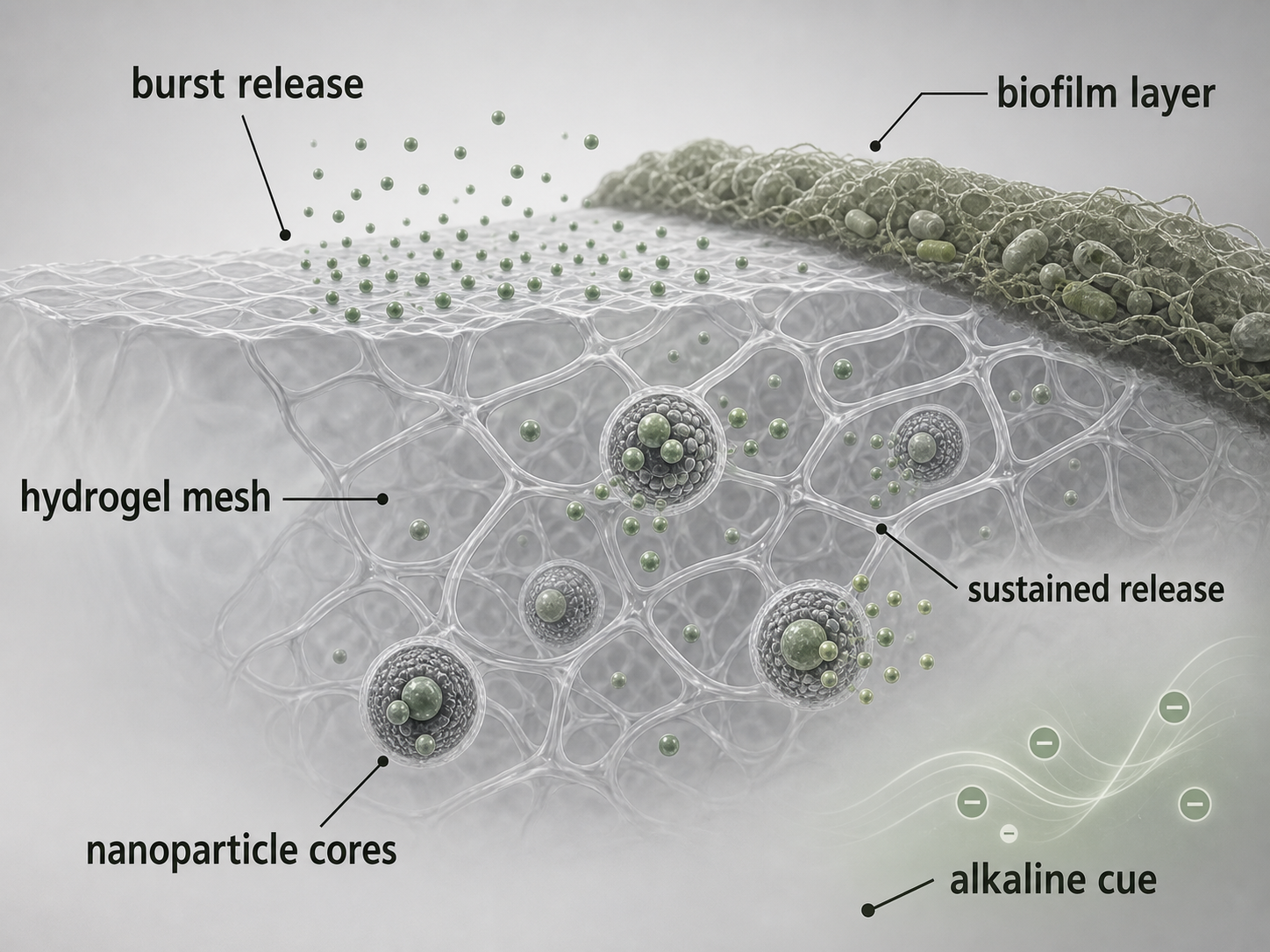
The 2024 thermosensitive hydrogel study used a PECT hydrogel to create programmed dual-octenidine release. Hydrophilic octenidine dihydrochloride was placed in the hydrophilic part of the hydrogel for early burst release. Hydrophobic octenidine was loaded into PECT nanoparticles for slower sustained release. Calcium hydroxide was incorporated to create an alkaline environment.
The model then tested antibiofilm performance in root-canal systems and an apical-periodontitis rat model. The source is useful because it shows how carrier architecture changes the question. A burst-and-sustain hydrogel is not the same experiment as a brief irrigant exposure, a planktonic MIC plate, or a historical skin-degerming application.
For method interpretation, ask what exposure curve the system created:
- Was octenidine freely dissolved at the start?
- Was it released from a gel, nanoparticle, spray, wound gel, or other carrier?
- Was the endpoint measured during burst release, after sustained release, or after the carrier changed?
- Did alkaline pH, degradation, or matrix interaction change local availability?
Hydrogel wording should stay just as specific. A hydrogel result is not a generic result for every gel, rinse, depot, or wound product. It is a result for a defined carrier architecture, loaded active form, release profile, matrix, organism model, and endpoint. The word “hydrogel” names the delivery system; it does not replace the release data or the biological model.
The useful comparison is therefore not “hydrogel versus no hydrogel” in the abstract. It is whether the carrier created early release, sustained release, retained activity, removable material, or a different local exposure window in that model. That makes release-system evidence valuable, but only when the release curve and endpoint stay attached.
Analytical Methods Are Part Of The Evidence
Analytical verification matters because microbiology cannot fix an uncertain formulation measurement.
The 2026 RP-HPLC paper developed a simultaneous method for octenidine dihydrochloride and phenoxyethanol in antiseptic formulations. It used a cyanopropyl column, an acetonitrile-water mobile phase with 0.1% trifluoroacetic acid in each phase, a 60:40 ratio, 1 mL/min flow, and UV detection at 270 nm. The reported linear ranges were 0.5 to 3.0 micrograms/mL for octenidine dihydrochloride and 3.0 to 50.0 micrograms/mL for phenoxyethanol, with an approximately 8-minute isocratic run.
That source does not answer whether a formulation works in a wound, mouth, canal, or biofilm. It answers a different but necessary question: whether the analytes can be separated and quantified in the tested matrices. When an antimicrobial result depends on a formulated product, an assay reader should ask whether the active concentration, co-ingredient concentration, matrix interference, and sample-preparation steps were verified.
Endpoint Choice Decides What The Claim Can Say
Octenidine studies often use endpoints that sound similar but mean different things:
- MIC or IC100% in broth growth measurement.
- Death kinetics over a stated contact time.
- CFU recovered from dentine chips.
- Log-transformed CFU after neutralization.
- Biofilm architecture by microscopy.
- Release percentage from a carrier.
- HPLC assay of formulation content.
- Animal-model inflammation or tissue findings.
None of these endpoints automatically outranks the others. They answer different questions. A CFU result after 1.5 minutes in an extracted-tooth model cannot be merged with a 20-hour microdilution growth curve as if both were the same “octenidine efficacy” endpoint. A release curve cannot be rewritten as a clinical outcome. A validated HPLC assay supports composition and measurement, not patient benefit.
A Practical Reading Checklist
Before comparing two octenidine findings, name the interface:
- Chemical term: octenidine, octenidine hydrochloride, octenidine dihydrochloride, or a finished product.
- Solvent or vehicle: water, PBS, Hepes, gel, spray, hydrogel, nanoparticle system, or commercial formulation.
- Organism and state: planktonic culture, single-species biofilm, multispecies biofilm, dentine-associated cells, or animal model.
- Inoculum: measured by OD, colony count, total-cell staining, McFarland standard, or another method.
- Organic load: protein, serum, dentine debris, biofilm matrix, cell debris, or none reported.
- Exposure: concentration, contact time, release profile, replenishment, irrigation, or repeated passage.
- Neutralization and carryover: whether the active was stopped, diluted, or allowed to continue acting.
- Endpoint: MIC, MBC, IC100%, death kinetics, CFU recovery, microscopy, release, HPLC quantification, or model pathology.
When those items are visible, apparently conflicting results often become less mysterious. The studies may not disagree about octenidine as much as they ask different questions at different chemical interfaces.
Useful Wording
For researcher-facing copy, the safest wording keeps the method attached:
- “In this E. coli microdilution system, octenidine activity varied with solvent and bacterial cell count.”
- “In this extracted-tooth model, the octenidine-containing final rinse was tested after defined contamination, irrigation, neutralization, dentine-chip sampling, and CFU counting.”
- “In this hydrogel model, dual release changed the exposure profile by combining early hydrophilic octenidine release with slower hydrophobic octenidine release from nanoparticles.”
- “In this HPLC method, octenidine dihydrochloride and phenoxyethanol were separated and quantified in tested formulation matrices.”
Avoid wording that hides the interface:
- “Octenidine is always stronger in water.”
- “Octenidine resistance was shown because growth occurred.”
- “A hydrogel result proves a rinse result.”
- “An HPLC method proves clinical effectiveness.”
- “One organism, one protein load, or one biofilm model represents all use contexts.”
Sources And Review
This article uses experimental setup, microbicidal activity, endodontic model, controlled-release hydrogel, analytical-method validation, and membrane-mechanism literature.
Editorial review focused on keeping each claim tied to the source model: solvent and inoculum effects from the 2022 E. coli setup paper; historical organism-kill and skin-degerming context from the 1985 microbicidal study; root-canal final-rinse boundaries from the 2025 extracted-tooth study; MIC, MBC, contact-time, and CFU-recovery endpoint boundaries; release-design interpretation from the 2024 PECT hydrogel study; analytical verification from the 2026 RP-HPLC paper; and membrane-interface caution from the 2021 membrane-mechanism paper. Last reviewed: 2026-05-28.